Coarctation of the Aorta
Quick Facts
- In coarctation of the aorta, a specific part of the aorta is narrowed or constricted.
- CoA can cause high blood pressure in the upper part of the body or low blood pressure in the lower part of the body. It can also cause heart failure.
- Coarctation can be repaired.
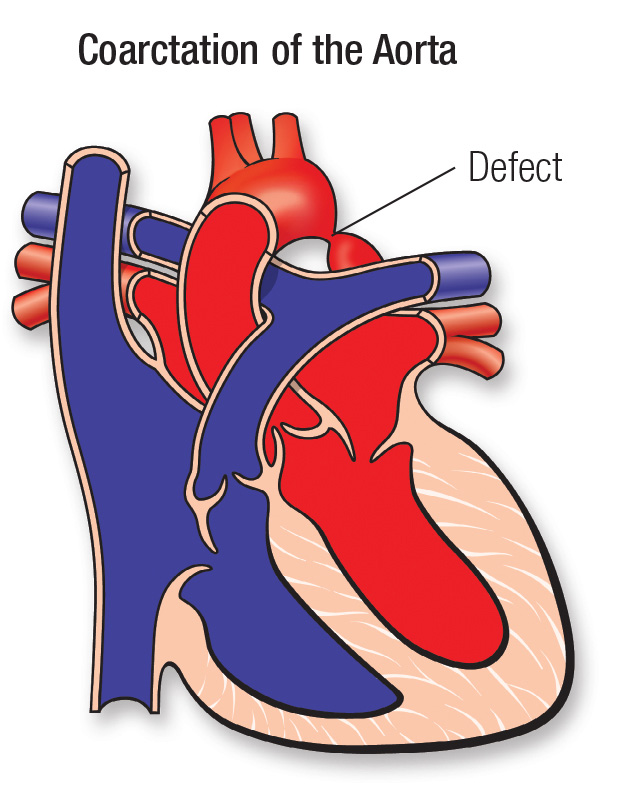
What is coarctation of the aorta?
In this condition, a specific part of the aorta (the main artery that carries blood from the heart to the body) is narrowed or constricted.
This narrowing affects blood flow where the arteries branch out to carry blood along separate vessels to the upper and lower parts of the body. CoA can cause high blood pressure in the upper part of the body or low blood pressure in the lower part of the body. It can also cause heart failure.
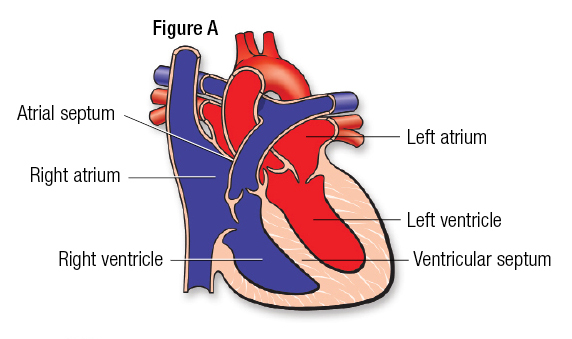
The heart has four chambers. The upper two chambers are the atria, and the lower two are the ventricles (Figure A). The chambers are separated by a wall of tissue called the septum. Blood is pumped through the chambers, aided by four heart valves. The valves open and close to let the blood flow in only one direction.
What causes CoA?
In most children, the cause isn’t known. Some children can have other heart defects along with coarctation.
The narrowing often occurs near the ductus arteriosus. In some cases, tissue from the ductus extends into the aorta and constricts as the ductus closes after birth, leading to narrowing.
How does CoA affect the heart?
Coarctation obstructs blood flow from the heart to the lower part of the body. Blood pressure increases above the constriction. The left ventricle must generate higher blood pressure than normal to push blood through the narrowed area. This can cause thickening (hypertrophy) and damage to the overworked heart muscle.
CoA is associated with another heart defect known as bicuspid aortic valve, where there are two aortic valve leaflets instead of three. This condition can be seen in up to 85% of patients with CoA.
What are the symptoms of CoA?
In newborns, there are usually no symptoms at birth, but they can develop as early as the first week. Some babies develop heart failure or high blood pressure.
When the narrowing is mild, the heart doesn’t need to work as hard, and symptoms might not appear. In some children and teens, coarctation is diagnosed later, often after high blood pressure is detected during a routine checkup.
Some adults with CoA may have headaches, kidney problems, repeated pregnancy loss or tiredness in their legs when active. However, these symptoms are common and often happen for reasons not related to CoA.
How can CoA be treated?
An infant with a severe coarctation should have a surgical procedure to relieve the obstruction. This may relieve heart failure in infancy and prevent problems later, such as developing high blood pressure as an adult because of the CoA.
A surgeon doesn’t have to open the heart to repair the defect. It can be fixed in several ways, including:
- Removing the narrowed segment of the aorta
- Sewing a patch over the narrowed section using part of the blood vessel to the arm or a graft of synthetic material
Cardiac catheter balloon dilation and stent placement can also be used. These are more commonly done in older patients and in patients with recurrent coarctation after surgery. In this case, the balloon may stretch the narrowed area, while the stent provides stiff support to prevent the vessel from returning to its smaller size.

CoA in children: What families need to know
What activities can my child do?
If the coarctation has been repaired and there is no remaining narrowing or high blood pressure, your child may not need limits on physical activity. Many children can safely take part in normal activities.
Some children may need to limit activity if they still have narrowing, high blood pressure, heart muscle changes or other heart conditions. Your child’s pediatric cardiologist can help guide which activities are safe.
What will my child need in the future?
The outlook after surgery is favorable, but long-term follow-up by a pediatric cardiologist is needed. In rare cases, CoA may recur. If this happens, another procedure to relieve the narrowing may be needed. Also, blood pressure may stay high even when the aorta’s narrowing has been repaired.
What about preventing endocarditis?
Children with CoA may risk developing endocarditis, an infection of the heart. Your child’s cardiologist may recommend that your child take antibiotics before certain dental procedures for a period of time after coarctation repair.
CoA in adults: What to expect
What if CoA was repaired in childhood?
Most people who were treated for CoA before 1985 had surgery. The type of repair depended on the location and severity of the narrowing. Some younger adults may have had a repair in a catheterization lab (referred to as interventional or therapeutic catheterization), where the narrowing was expanded by a balloon inserted through a small hole in the leg. Often, a metal stent was left in place to hold the area open. This may also be an option if further narrowing occurs in an adult.
If CoA is still present, should it be repaired in adulthood?
Coarctation can be repaired at any age. The timing of treatment depends on its severity, symptoms and blood pressure effects. Teens and adults can often be treated with cardiac catheterization.
What CoA problems are common in adults?
High blood pressure is the most common long-term problem for adults who have had CoA repaired. It is more likely if the repair was done after age 5.
Patients treated in childhood can also develop narrowing of the aorta again, called recoarctation. They may need catheterization. Some people with recoarctation may not have noticeable symptoms, but it can still lead to high blood pressure or other complications. Regular check-ups are important to detect and treat these problems early.
In some cases, the aorta can narrow again, or other areas of the aorta can widen. These areas, called aneurysms, may need treatment. Adults with repaired coarctation may also have a higher risk of heart disease or problems with blood vessels in the brain. Regular follow-up care helps find and manage these issues early.
Ongoing Care
If you have CoA, you should have regular follow-up visits with a cardiologist experienced in congenital heart disease. The frequency of visits depends on your condition.
At these visits, your blood pressure should be checked in the arms and legs. Many people need medications to help control blood pressure. These often include beta blockers such as atenolol or metoprolol.
You will also need regular imaging tests to check your aorta. These tests may include an echocardiography or MRI. A CT scan can also show the aorta well and may be used when an MRI is not suitable, although it involves radiation and is not typically used for routine follow-up care.
If you need any type of non-heart surgery or invasive procedure, talk with your congenital heart disease cardiologist ahead of time.
Activity
Most activities are safe and encouraged. In some cases, very heavy exercises that involve straining may be a concern, especially for people who have an enlarged aorta. These activities can raise blood pressure quickly.
Endocarditis prevention
Infection of a coarctation is rare. More often, an infection may involve an abnormal aortic valve that occurs along with coarctation. Good oral care is important for everyone and can help lower the risk of infection.
Pregnancy
Many women who have a repaired CoA can have a pregnancy with low risk. Risk may be higher if there’s still some remaining narrowing of the aorta, high blood pressure or enlarged areas of the aorta.
It’s a good idea to plan ahead and have a full checkup before becoming pregnant. This may include imaging tests to look at the aorta and help find any issues early. Managing issues before pregnancy can help support a healthier pregnancy.
When is more surgery needed?
Whether you need another procedure depends mostly on your blood pressure in your arms and legs. This is checked when you’re resting and sometimes during exercise.
If the blood pressure in your arms and legs is normal and about the same, you likely will not need more treatment. If the blood pressure in your arms is high and much higher than in your legs, more treatment might be needed.
When treatment is needed, many health care professionals use a catheter-based procedure instead of surgery.





